The shoulder has the greatest motion of any joint in the body. This motion puts extreme stress on the joint, tendons, and muscles that stabilize the shoulder. Dr. Ryan Smart, SOS Shoulder and Sports Medicine Specialist, discusses keeping your shoulders working properly and pain free.
By. L. Ryan Smart
Shoulder pain is complex. It is complex primarily because of the anatomy of the shoulder and the surrounding structures. The shoulder has the greatest motion of any joint in the body. This motion puts extreme stress on the joint, tendons, and muscles that stabilize it.
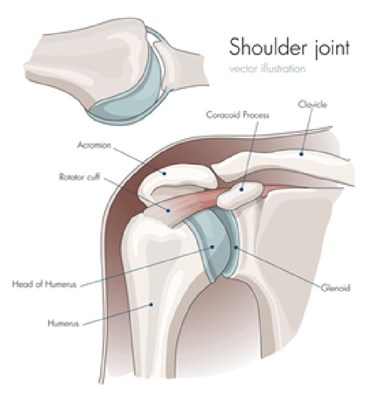
The glenoid (aka socket) of the shoulder is very flat, like a saucer dish, allowing 180 degrees of motion. The humeral head (aka ball) is smooth and round also permitting extreme motion. The labrum (the gasket that rims the socket) and the glenohumeral ligaments statically support the joint and give it stability. The 4 rotator cuff muscles through their tendinous connections onto the humeral head dynamically stabilize the joint. The scapula (aka shoulder blade) is the same bone that becomes the glenoid. It has 17 muscles that attach to it providing it stability!
All of these muscles must work in concert to keep the shoulder working properly and pain free. In addition, the cervical spine (aka neck) can also contribute to shoulder pain as many of the nerves that come out the neck go straight to the shoulder. All of this makes diagnosing shoulder pain difficult and the orthopedic surgeon must have great mastery of the anatomy.
 Shoulder pain is typically age related. Pain in the younger population (<30) is commonly traumatically related. While pain in the over 30 cohort can be traumatic in origin, it is more frequently related to overuse or inflammation based.
Shoulder pain is typically age related. Pain in the younger population (<30) is commonly traumatically related. While pain in the over 30 cohort can be traumatic in origin, it is more frequently related to overuse or inflammation based.
Younger Shoulder Pain
Traumatic: Most commonly fracture of clavicle (collarbone), proximal humerus (upper arm bone), dislocation (bone comes out of the socket), separation (AC joint injury)
Overuse: Typically in overhead athlete: baseball, swimming, volleyball; pain from rotator cuff tendinitis, or scapula muscle dysfunction (scapulothoracic dyskinesia)
Older Shoulder Pain
Overuse: Rotator cuff pain - tendinitis, bursitis, or tear; impingement syndrome (rotator cuff tendon rubs against acromion bone that is the ceiling of shoulder), frozen shoulder (inflammation of the glenohumeral ligaments deep in shoulder; more commonly seen in diabetics or those with thyroid problems, but commonly occurs for no know reason (idiopathic)
Traumatic: Fall that results in rotator cuff tear (commonly seen in CNY with slip and falls on ice landing on shoulder or outstretched arm); fall that results in fracture

Many shoulder conditions present with similar complaints: nighttime pain, dull ache in upper arm bone, sharp pain with certain movements, pain when lying on that shoulder, etc. It is extremely important for the physician to sort out the true cause of the patient's pain based on their history and exam. Was there a trauma that started the pain, or did it start on its own (ie I slept on it wrong)? Is the shoulder stiff with both active and passive motion (frozen shoulder or arthritis) or just active motion (rotator cuff problem)?
In order to properly treat a patient, the physician must make an accurate diagnosis. Sometimes this takes further work-up with an X-ray and/or an MRI. X-rays show bones. They give the physician an idea of the amount of arthritis in the joint or any other bony problem. MRIs show primarily soft tissue structures particularly the rotator cuff tendons. You can see if there is any structural damage to them (aka tears).
Often physicians will have patients try a short period of anti-inflammatory medicine (ibuprofen, Advil, Aleve, Motrin, etc) to diminish pain and rehab the shoulder with physical therapy to get the shoulder in proper working order. Other times we will try a cortisone shot into certain anatomic locations to help diagnose a problem and treat it at the same time. Physical therapy can really benefit patients and often can help make surgery unnecessary by getting the shoulder and the surrounding structures back in working order. Occasionally, if all nonsurgical measures fail, surgery can be used to help treat the problem. Arthroscopy (minimal invasive surgery) of the shoulder is a great way to look inside the joint and confirm the problem and fix it. This is an ideal way to repair torn rotator cuff tendons, remove arthritis or bone spurs, fix labral tears, release frozen shoulders, etc.
Physical therapy is commonly needed to rehab the shoulder after surgery. The most common complication after shoulder surgery/arthroscopy is stiffness. PT helps minimize it and maximize patient's outcomes. Typically shoulder recovery after surgery can range from 6 weeks to 6 months for full recovery depending on what was done. A quick cleanout surgery is a relatively quick recovery of 2-3 weeks of surgical pain with most patients being fairly pain free and functional by 6 weeks. Rotator cuff repair surgery takes longer to heal because the tendon needs to heal back to the bone which typically requires 3 months to happen. A sling is usually worn after surgery. Depending on what was actually done it can vary from 2-3 weeks to 10 weeks.
Hope this helps better understand shoulder problems and how an orthopedic surgeon that specializes in them thinks about it.